


As Predicted, Vexxine Efficacy Shrinks Once Out Of The Hands Of Pharmaceuticals
Part The First: Observations
How good is the Pfizer vex in practice? Ask them---or any Expert or ruler---and they will say...well, let's not ask them what they would say. It would only encourage them to tell more "noble" lies.
We can recall back to last December, when the first safety and efficacy data was released by the FDA for the Pfizer vex based on their (Pfizer's) controlled trials. They were touting numbers like 95% for efficacy. Which sounds terrific. But I said this about that huge effect:
As I’ve said before, trial numbers in medical experiments always look better than real-life numbers, and I’d bet good money these numbers will shrink. I have no idea by how much. I’d be (pleasantly) surprised if in real life it was much north of 50%.
Let's see if we can count that prediction as a victory.
Enter the paper "Six Month Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine" by Stephen J Thomas and a legion of others.
They looked at about 44 thousand 16+ year olds, plus another 2 thousand 12-15 year olds. Two doses for half, and a placebo for the other half, with shots 21 days apart. And they were all looked at up through 6 months afterward for outcomes like infections and side effects, including death.
At the end, 21,926 were in the vex group and 21,921 in the placebo: 15 died in the vex group, and 14 in the placebo group, by of all sorts of causes. Only 1 died in the vex group of "COVID-19 Pneumonia", a fair thing to track because, like flu, it's not the disease that gets you most often, it's the resulting pneumonia. And 2 died of the coronadoom in the placebo group.
They also tracked infections, but these are of almost no interest. Not to us, dear reader, especially since (1) vaccines can't stop you from being infected, and (b) everybody is going to get this thing eventually, and for most it's nothing to sweat over, if it's even noticed. So we'll look at the times when people should sweat, which is to say, at deaths.
Overall, that's 1/21926 = 0.000046 in the vex groups versus 2/21921 = 0.000091, for a grand savings of 0.000046. Or an actual difference of 0.0046%.
That's what the vex does, crudely. Buys 0.0046% improvement in deaths due to the doom.
Because it sounds better, they would report the relative improvement, which is 1 - (1/21926) / (2/21921) = 0.5, or--ta da!---50%.
I humbly accept your thanks of an accurate prediction.
Part The Second: Projections
Now theses numbers are absolute in the sense they happened to these 44 thousand people, assuming all the measurements were accurate. The rates of improvement, given this clean measurement assumption, are certain.
But not if we apply them to new people. Then there is uncertainty. We can, if we like, though it's not necessary, quantify that uncertainty. Let's do so, for fun.
First recall all models only say what they are told to say. Here is what we are telling our model to say.
We've discussed it dozens of times before, so I'll just state that given just the assumption we have no idea how many "successes" (deaths) or "failures" (surviving; hey, we're on the pharmaceuticals side here) there will be in a new group of people, other than it can be any number between 0 and the total, then our predictive probability is a beta-binomial.
There is another tacit assumption which is crucial. It is that this new batch of people be like the old batch of 44,000 in a causal sense. That is, the new group must share the same causal connections between the bug, vex, disease and death as the old one; this includes the time frame, which is 6 months. Probability in the predictive way isn't magic like in classical stats: probability for us has no power. Cause does. We don't know all the causes, so we use probability.
All right, what future group is like the past group causally?
I don't know.
The study looked at people in Argentina, Brazil, South Africa, Germany, and Turkey. Maybe we can apply our model to Americans in the coming six months. I'm not sure. American coronadoom medicine has been crappier, judged by outcomes, compared to other parts of the world.
And then the coming six months starts when there is a decrease in death because of other causes, and which will see a rise in new deaths because of late fall.
Plus, this study only looked at the Pfizer jab, and in the USA there are other options.
Are all these differences important? Don't know. Let's push on.
According to the CDC, as of 1 October, at 10 of the clock, 184,469,107 Americans ages 12+ were "fully" vexxed, which, they say, was 65.1% of all people in this age group. That leaves 98,893,577 un-"fully" vexxed. Some of these folks had one shot of the two-shot vexxes. In which group to put them? Don't know. How about the un-"fully" vexxed? Some 214 thousand have at least one shot.
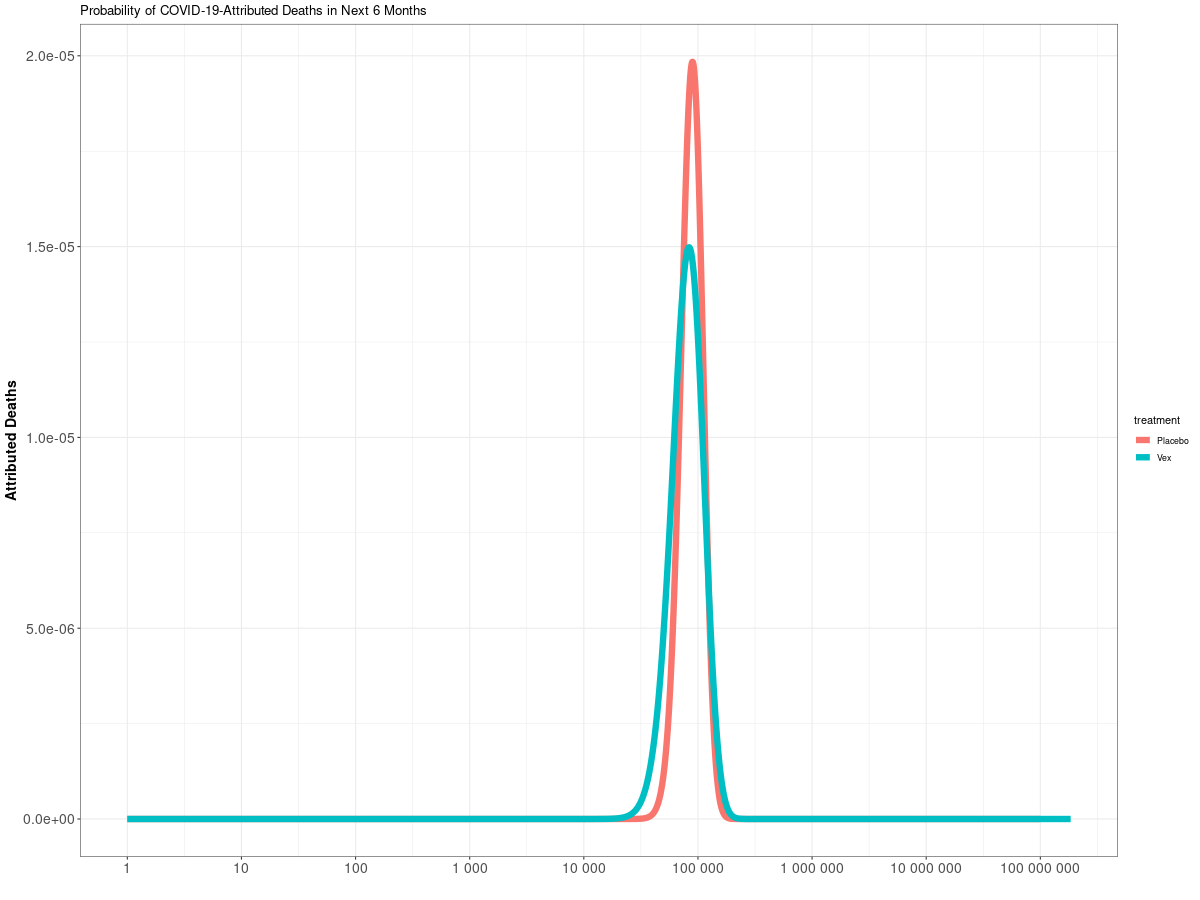
Here's the first prediction:
If this model's premises align with Reality, then in the next size months about the same number of "fully" vexxed as un-"fully" vexxed will die. Call it about 10,000 in each group, with a fairly large window. But also recall the number of "fully" vexxed to un-"fully" vexxed is just under two to one.
Right away we see this is way off. Week before last had about 5,000 doom deaths, says the CDC, with numbers dropping. Still, twenty thousand seems like a pretty bad undercount for six months out. 26 weeks at 5k per week is 130 thousand, but again that 5K is dropping per week. Recall last October-March saw about 352 thousand die from the doom.
So maybe a good window is 50 - 300 thousand. Don't forget, back in olden days, about 200 thousand died every year of flu+pneumonia, mostly in these coming six months, even with vexxines. Since few are dying of flu anymore, that window is a good guess.
In any case, it's clear with these assumptions that our model is likely off by an order of magnitude. Here's the official weekly deaths:
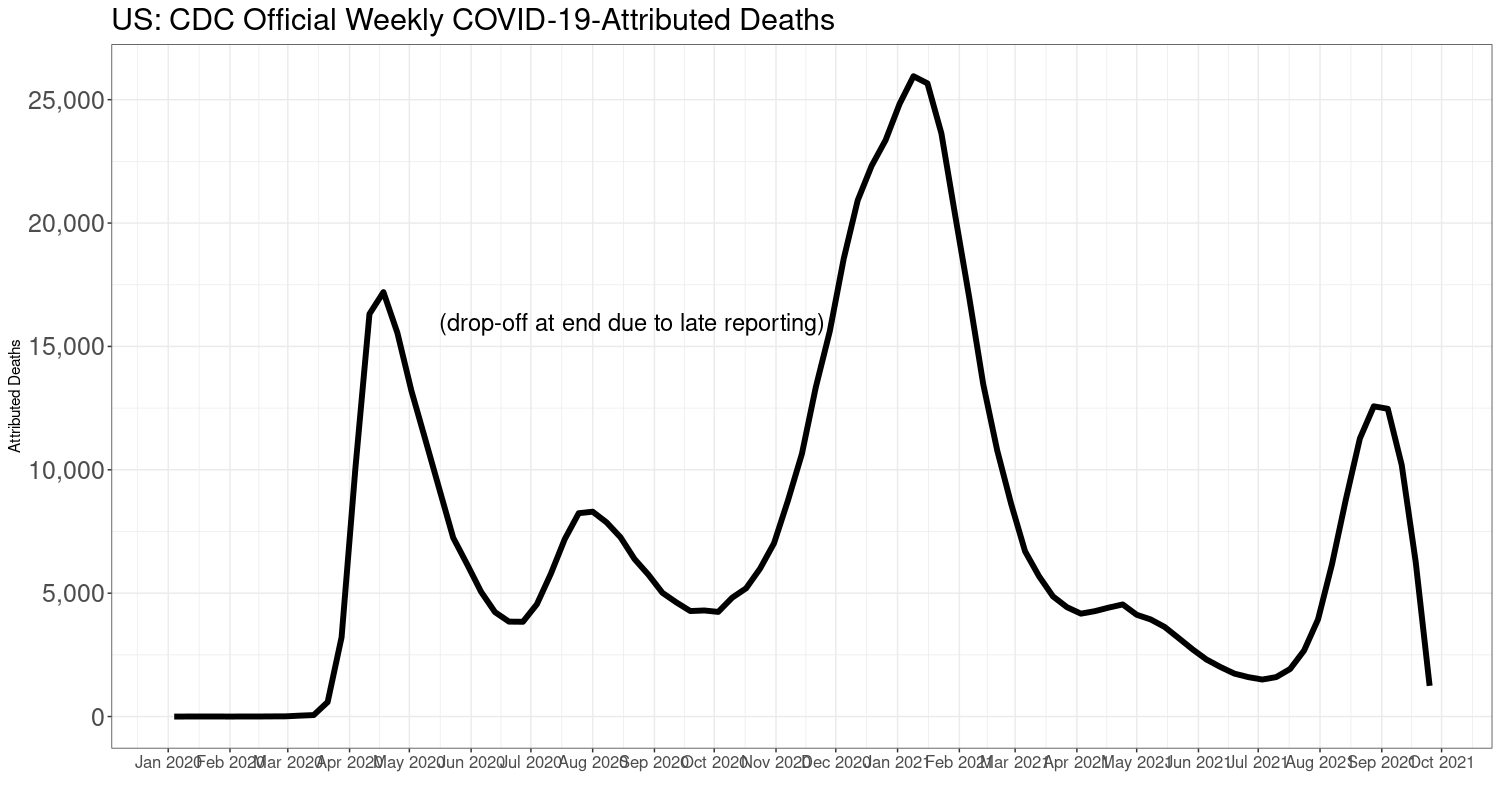
On the other hand, if deaths do keep dropping, then we'll be closer. However, they'll still pick up again in late fall, as sure as Congresspersons accept bribes.
This means, probably, that these other countries are not like the US in at least one causal sense. Could be the quality of care (widely variable), or the physical state of the people (lousy, drugged up; have you seen our many, many drive-up prescription pick-up windows?).
Let's try this. Let's assume the same vex/placebo--1/2 ratio but up the dead bodies in each group to reach American levels. We have to do this guessing because the CDC isn't giving us actual numbers to use. Busy people, I guess. Here's 10 dead in the vex group, and 20 in the placebo: we assume these are in the old data.
This brings us in line with about 200 thousand dead in 6 months. Also notice that more vexxed will die than unvexxed. But proportionally more unvexxed will die.
This assumption gives 10/22085 = 0.00045 dead in the vex group, and 20/22080 = 0.00091 in the unvexxed. I mean, this assumes we would have seen this number if the same experiment by our authors was done in the USA.
That's maybe not so bad as far as assumptions go. The population fatality rate for 85+ in the last two years was 0.028; for for 75-84 was 0.01; for 65-74 was 0.0045; for 55-64 was 0.002; for 45-54 was 0.00084; for 35-44 was 0.0003. And that's enough, because so few died under 35.
You can see that these numbers aren't far off from our imagined experiment.
There's too many ifs and buts for this model to be taken seriously. It does show how hard it is to do these kinds of things. Still, it has some aspects that might turn out interesting.
The one prediction that will likely hold is that more vexxed than unvexxed will die in the next 6 months. Mostly because this group far outnumbers the unvexxed, and because the vex isn't that great.
Check back again in 6 months and see how we did.
Subscribe or donate to support this site and its wholly independent host using credit card or PayPal click here