


Three New Hilarious Papers On The Coronadoom Vaccine
Listen to the podcast at YouTube (sorry, the Reality censors there won’t allow this video; It’s Science!), Bitchute, or Gab.
Three papers on the All Holy Vex—praise it!
College Mandates
Before we get to it, do you know of any college, university or other indoctrination center that still mandates the coronadoom vex for students, the group of adults least likely to suffer from the doom itself?
Peer-reviewed paper is “COVID-19 vaccine boosters for young adults: a risk benefit assessment and ethical analysis of mandate policies at universities” by Kevin Bardosh and others in the BMJ’s Journal of Medical Ethics.
Abstract (here and elsewhere with my paragraphifications and emphasis; I also put commas in the numbers in the American way):
In 2022, students at North American universities with third-dose COVID-19 vaccine mandates risk disenrolment if unvaccinated.
To assess the appropriateness of booster mandates in this age group, we combine empirical risk-benefit assessment and ethical analysis.
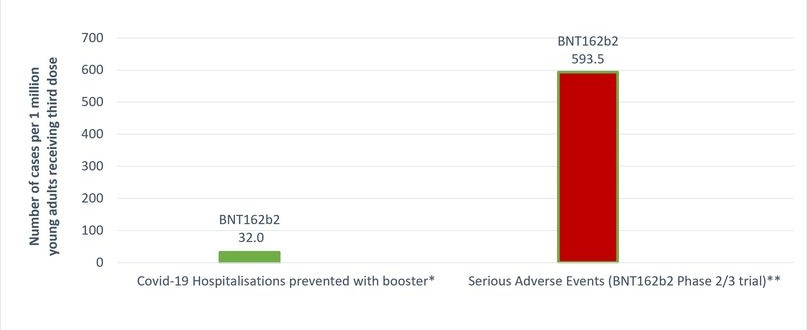
To prevent one COVID-19 hospitalisation over a 6-month period, we estimate that 31,207–42,836 young adults aged 18–29 years must receive a third mRNA vaccine.
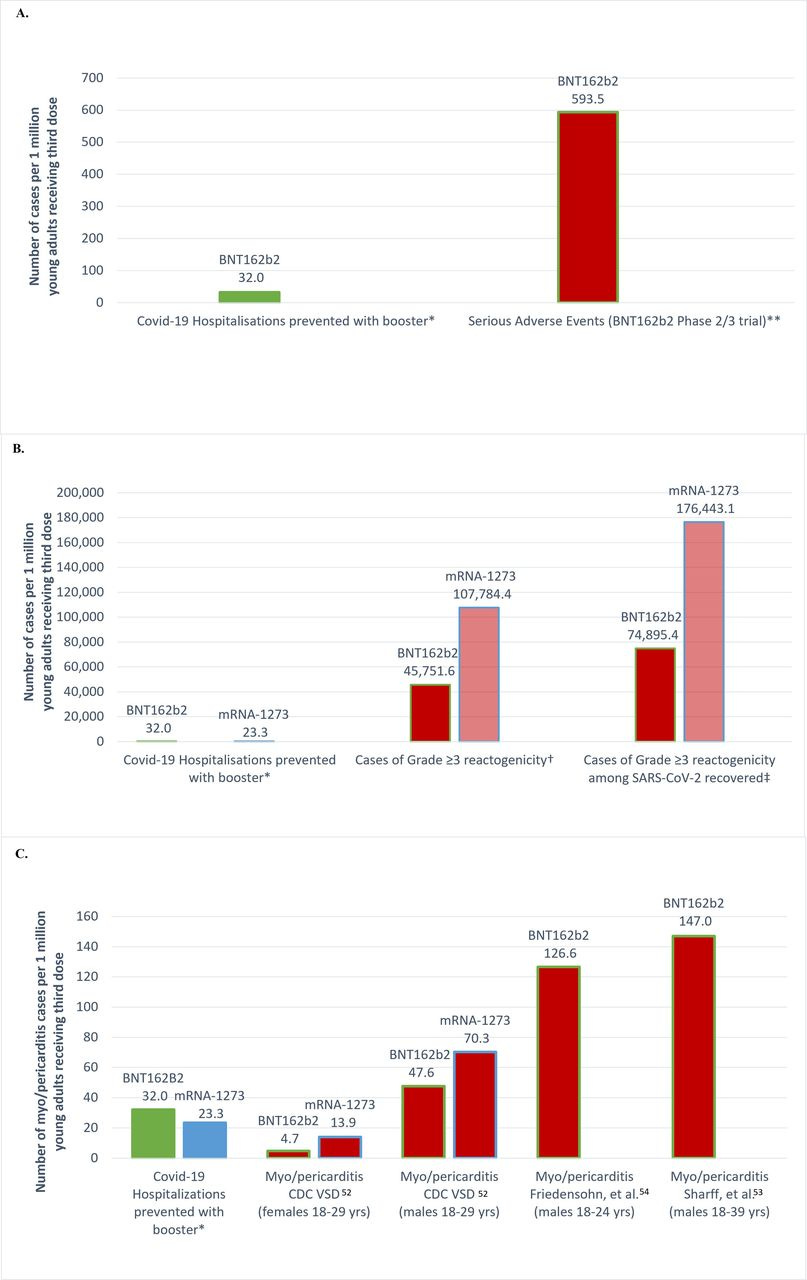
Booster mandates in young adults are expected to cause a net harm: per COVID-19 hospitalisation prevented, we anticipate at least 18.5 serious adverse events from mRNA vaccines, including 1.5–4.6 booster-associated myopericarditis cases in males (typically requiring hospitalisation).
We also anticipate 1430–4626 cases of grade ≥3 reactogenicity interfering with daily activities (although typically not requiring hospitalisation).
University booster mandates are unethical because they: (1) are not based on an updated (Omicron era) stratified risk-benefit assessment for this age group; (2) may result in a net harm to healthy young adults; (3) are not proportionate: expected harms are not outweighed by public health benefits given modest and transient effectiveness of vaccines against transmission; (4) violate the reciprocity principle because serious vaccine-related harms are not reliably compensated due to gaps in vaccine injury schemes; and (5) may result in wider social harms.
We consider counterarguments including efforts to increase safety on campus but find these are fraught with limitations and little scientific support. Finally, we discuss the policy relevance of our analysis for primary series COVID-19 vaccine mandates.
Big Fig:
Try this fun experiment. Send this (and the others below) paper to your favorite college administrator and say, “See? You should drop the mandates.”
Wear something plastic or discardable if you’re doing this in person.
And, say, remember when myocarditis was a conspiracy theory?
Extra Vexatious
This one is from our friend Eugyppius: Cleveland study conducted to demonstrate the clinical effectiveness of the bivalent vaccines accidentally finds that the risk of Covid-19 infection increases with each prior vaccination. Read his description; subscribe to his Substack.
The paper has a rather dry title, a signal the authors know their data will be “controversial”, and they don’t want to be blamed for its logical implications, is “Effectiveness of the Coronavirus Disease 2019 (COVID-19) Bivalent Vaccine” by Nabin K. Shrestha and others.
Sample size north of 51,000.
Here’s their Big Fig: “Simon-Makuch plot comparing the cumulative incidence of COVID-19 for subjects stratified by the number of COVID-19 vaccine doses previously received.”
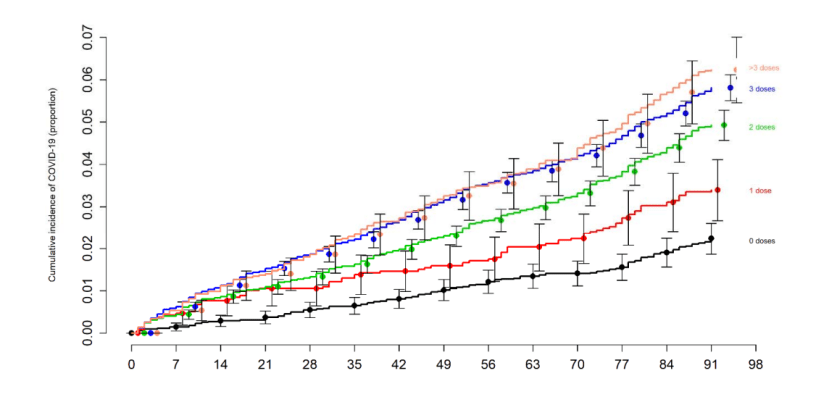
The more doses, the more likely the infection. Hilarious. (Read E’s article for discussions about potential biases etc.)
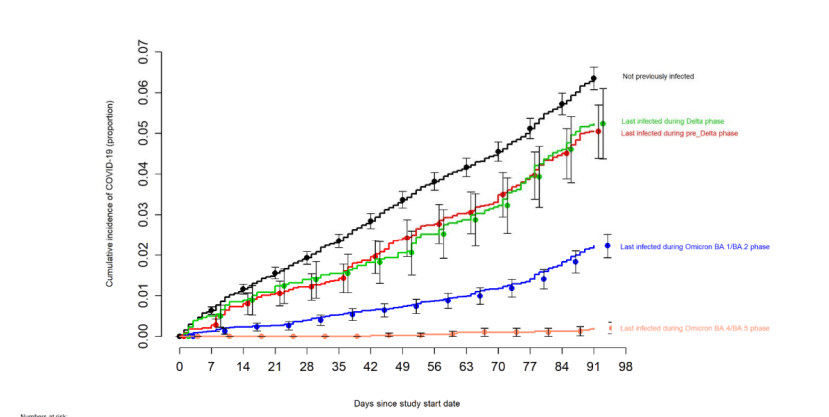
Big Fig 2 shows the Expert scientists at the CDC are—amazing as this will seem—wrong again, and that naturally acquired immunity is superior to the vex.
Incidentally, the Experts at CDC still requires foreigners to be “fully” vexxed to travel to the USA. Unless they enter illegally, then then don’t require it. And they don’t require citizens to vex. Which makes their policy both inconsistent and anti-science.
This is a good place to remind us of the wisdom of our rulers:

You Say Thromboembolic, I Say Thrombocytopenic: Let’s Call The Whole Thing Off
Peer-reviewed paper is “Analysis of Thromboembolic and Thrombocytopenic Events After the AZD1222, BNT162b2, and MRNA-1273 COVID-19 Vaccines in 3 Nordic Countries” by Jacob Dag Berild and others in JAMA Network Open.
Let’s skip right to the Findings: “In this self-controlled case series, AZD1222 was associated with increased rates of cerebral venous thrombosis and thrombocytopenia in 3 Nordic countries.”
More fully (and this was a huge study):
In this self-controlled case series, there was an increased rate of hospital contacts because of coagulation disorders and cerebrovascular disease, especially for thrombocytopenia and cerebral venous thrombosis, following vaccination with AZD1222. Although increased rates of several thromboembolic and thrombocytopenic outcomes following BNT162b2 and mRNA-1273 vaccination were observed, these increases were less than the rates observed after AZD1222, and sensitivity analyses were not consistent.
Golly.
Get your boosters yet, citizen?
The sheer number of studies showing the utter lack of effectiveness of the vex is astounding. And yet it won’t make a bit of difference to university administrators, government bureaucrats or world leaders. Quadrupling (quintupling, etc.) down on stupidity is inevitable. None of them can admit how very wrong they are and were, the cognitive dissonance won’t allow it.
Thanks! That BMJ article is simply a gold mine of quotes and links. To mention just a few, myocarditis rates according to various studies vs official statements, hospitalization rates for post-v myocarditis, and recovery rates (very bad) for post-v myocarditis. I don't see how a v-propagandist could survive a link like that.